Prevalence and incidence are two of the most commonly used terms in health reports, research papers, news articles, and policy discussions. They are often mentioned together, sometimes mixed up, and occasionally used as if they mean the same thing.
For rare diseases, misunderstanding these terms can distort perceptions of how common a condition is, how many people are living with it, and how urgently resources are needed. For patients and families, this confusion can also shape expectations about diagnosis, research activity, and available support.
Understanding what prevalence and incidence actually mean, and how they differ, is essential for interpreting health information accurately.
Before looking at the terms themselves, it helps to understand why these measures exist in the first place.
Healthcare systems, researchers, and policymakers need reliable ways to describe how diseases affect people. They need to know how many people are living with a condition right now, how often new cases appear, and how these patterns change over time.
Prevalence and incidence answer different questions. Both are important, but they serve different purposes.
Prevalence describes how many people are living with a condition at a specific point in time or over a defined period.
It answers the question: how widespread is this condition right now?
Prevalence includes everyone who has the condition, regardless of when they were diagnosed. Whether they were diagnosed yesterday or 30 years ago, and sometimes those whose disease is currently inactive but still present. It captures the total burden on healthcare, families, and society.
Prevalence is usually expressed as a proportion or rate, such as new cases per 1,000, 10,000, or 100,000 people.
There are two main ways in which prevalence is described.
Point prevalence is the proportion of a population that has a condition at a specific point in time. For example, how many people have a particular disease on a given date (e.g., January 1, 2026).
Period prevalence refers to the proportion of a population that has the condition at any time during a specified period, such as over a year.
Both are valid, but they answer slightly different questions. Point prevalence is more precise, while period prevalence captures a broader picture.
Incidence tells you how many new cases of a condition appear in a population over a specific period of time.
It answers the question:
Incidence is usually expressed as a rate, such as the number of new cases per year per 100,000 people.

Incidence can also be described in different ways.
An incidence rate accounts for both the number of new cases and the amount of time people are at risk. It is often used in research studies.
Cumulative incidence describes the proportion of a population that develops the condition over a specified period. It is easier to understand but less precise in some studies.
The choice depends on the purpose of the analysis.
Although related, prevalence and incidence measure different aspects of disease.
A condition can have a low incidence but high prevalence. This typically happens when a disease is rare but long-lasting. Once people are diagnosed, they live with the condition for many years.
Many rare genetic conditions fall into this category. Few new diagnoses each year, but the number of people living with the condition accumulates over time.
On the other hand, a condition can also have a high incidence but a low prevalence. This happens when a disease occurs frequently but is short-lived or rapidly resolved.
In rare diseases, the high-prevalence/low-incidence pattern is common. It explains why some conditions feel “rare” in terms of new cases but affect a noticeable number of people overall. Understanding this distinction is critical for interpreting statistics correctly.
Rare diseases are often defined using prevalence rather than incidence. In many regions, a disease is considered rare if it affects fewer than a specified number of people in the population at any given time. For example, affecting fewer than 1 in 2,000 people in Europe. In the United States, the Orphan Drug Act defines a rare disease as one affecting fewer than 200,000 people (FDA Orphan Drug Act).
This makes sense because prevalence reflects the ongoing burden on healthcare systems, support services, and communities.
However, focusing only on prevalence can obscure how often new cases arise. Some rare diseases have a higher incidence than expected because they are underdiagnosed or rapidly fatal.
Incidence helps show how many new families are affected each year, which matters for newborn screening, genetic counselling, and early intervention.
Both numbers give a fuller picture. Prevalence shows the current burden; incidence shows the rate of new cases and emerging needs.

Prevalence is shaped by two main factors: incidence (how often new cases occur) and duration (how long people live with the condition).
If treatment improves survival, prevalence may increase even if incidence stays the same (More people are living longer with the condition).
This is often seen as a success of medical progress, but it also increases demand for long-term care, services, and research.
In rare diseases, better supportive care and emerging therapies have turned many childhood conditions into lifelong ones, making adult services, transition planning, and long-term support increasingly important. For more context, see Orphanet and Rare Disease Watch’s article Orphan Drugs: From Neglect to Precision Medicine.
Incidence depends not only on how often a disease truly occurs, but also on how often it is diagnosed.
Improved awareness, better diagnostic tools, and screening programmes can increase reported incidence without any real change in disease biology.
This does not mean more people are becoming ill. It means more cases are being recognised.
In rare disease, advances in genetic testing have increased the incidence of many conditions simply by making diagnosis possible.
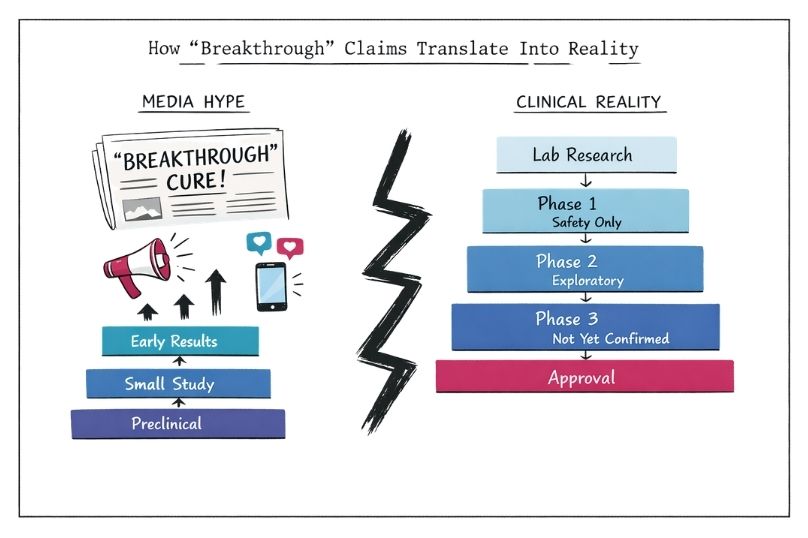
Media and public reports frequently blur the distinction between prevalence and incidence.
Headlines may claim that a disease is increasing without clarifying whether this refers to more people living with it, more new diagnoses, or both.
An “increase” in a condition might mean more people are living longer with it (higher prevalence), not that more people are getting it (higher incidence).
Low prevalence does not mean low need; many rare diseases affect few people but cause high individual impact.
Rising incidence does not always mean a disease is “spreading”; it can reflect better diagnosis.

Without this context, readers may assume a condition is spreading or becoming more common in a way that is misleading.
Clear use of prevalence and incidence helps prevent unnecessary worry or false reassurance.
Prevalence is often used to plan services. It helps estimate how many people need ongoing care, medication, therapy, or benefits.
Incidence is often used to plan prevention, screening, and early diagnosis. It helps identify where new cases are arising and whether patterns are changing.
Effective policy requires understanding both. Prevalence-based planning ensures services for those already diagnosed; incidence-based planning drives newborn screening, genetic testing, and diagnostic awareness.
In rare disease policy, balancing prevalence-based service planning with incidence-based diagnostic strategies is particularly important. Relying on one without the other can lead to misallocation of resources.

Measuring prevalence and incidence accurately in rare disease is difficult.
Many conditions are underdiagnosed or misdiagnosed for years. Some people never receive a definitive diagnosis. Others may be diagnosed years after symptoms begin.
Patient registries may be incomplete or inconsistent. Diagnostic criteria may change as knowledge evolves.
As a result, published figures should often be treated as estimates rather than precise counts.
It is common to see different prevalence or incidence figures for the same condition. This can reflect differences in study design, population, diagnostic criteria, or time period.
Geographic variation, access to healthcare, and data quality also play a role. When reading statistics, understanding how numbers were generated is often more important than the exact figure.
In research, prevalence studies help describe the burden of disease and identify affected populations. Incidence studies help identify risk factors, triggers, and early disease mechanisms.
Both are essential for building a complete picture, particularly in rare diseases where evidence is often limited. Researchers must choose the appropriate measure based on the question they are asking.
For patients and families affected by a rare disease, these terms influence more than just statistics.
Prevalence figures can affect how much research attention, funding, and availability of specialist expertise a condition receives. A very low-prevalence disease may struggle for resources, even if new cases appear regularly.
Incidence shows how many new families are joining the community each year, which matters not only for building awareness and support networks but also for strengthening data collection and advocacy.
Knowing the difference helps you interpret reports accurately, set realistic expectations, and advocate more effectively.
Numbers do not define lived experience, but they do influence systems, priorities, and perceptions. Understanding prevalence and incidence gives you clearer tools to navigate that world.
Get support and resources for rare diseases:
https://rarediseases.org/
https://www.eurordis.org/
Both are essential. Neither tells the full story alone.
In rare diseases, where numbers are small, but the needs are high, understanding this distinction helps ensure that data is used responsibly for better diagnosis, fairer resource allocation, and stronger support.
Prevalence and incidence are foundational concepts in understanding health and disease, yet they are often misunderstood or oversimplified. For rare disease communities, clarity matters. Misinterpreting these terms can affect everything from public perception to policy decisions and research investment.
At Rare Disease Watch, these concepts are not treated as abstract statistics. They are tools for understanding real lives, real needs, and real gaps in care.
Knowing what prevalence and incidence mean allows readers to engage more critically with health information and to ask better questions about what the numbers truly represent.