The management of a pediatric rare disease extends far beyond the immediate logistical requirements of hospital visits and medication schedules. While physical preparations such as maintaining a "hospital bag" are essential for acute situations, the long-term psychological burden on caregivers requires a different set of tools.
Statistics indicate that approximately 1 in 10 individuals are affected by one of the more than 7,000 known rare diseases, yet the resources for parental mental health often remain secondary to clinical patient care. Developing effective coping strategies for parents of children with rare diseases is a critical component of family-centered healthcare.
Research suggests that parents of children with complex medical needs experience higher rates of chronic stress, anxiety, and depression compared to the general population. Addressing the "mental game" of long-term caregiving ensures that the primary support system, the parents, remains resilient and capable of navigating the healthcare landscape for years or decades.
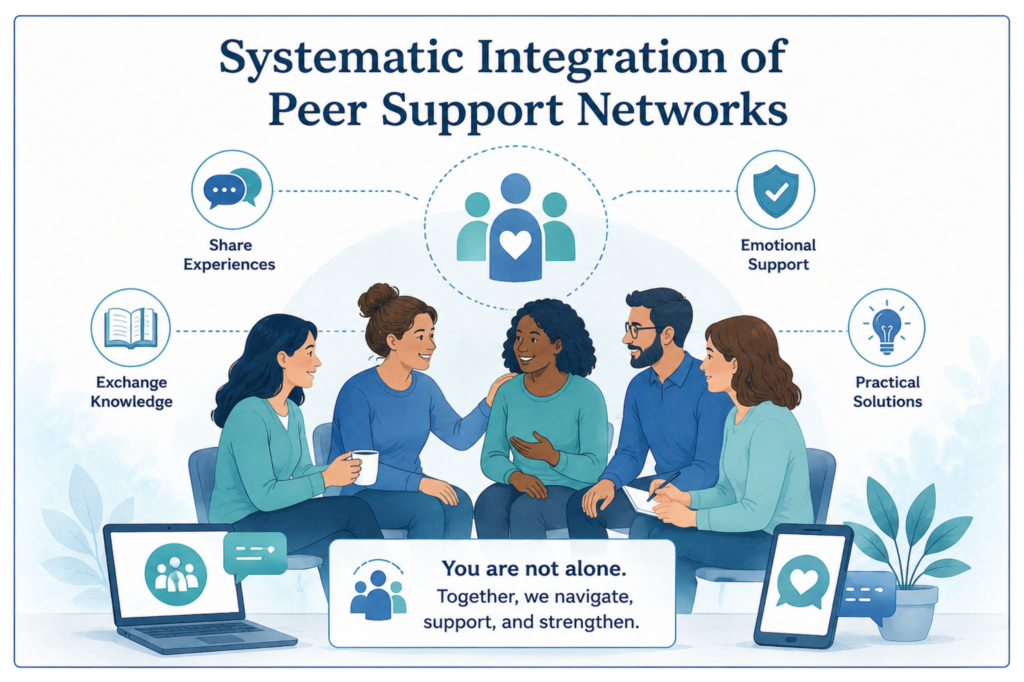
Isolation is one of the most significant psychological risks for parents in the rare disease community. Because many conditions are statistically infrequent, local medical professionals and social circles may lack specialized knowledge of the family's daily reality. Systematic integration into peer support networks serves as a vital intervention for reducing this sense of isolation.
Data shows that engaging with others who share a similar diagnostic journey can lower caregiver stress levels by providing validated experiential knowledge. These networks offer more than emotional comfort; they provide a database of practical solutions for navigating insurance hurdles, equipment sourcing, and school accommodations.
Parents should consult a directory of trusted organisations to find communities that align with their child’s specific diagnosis or broader category of disability. Participation in these groups allows parents to transition from being passive recipients of medical information to active participants in a knowledge-sharing ecosystem.
This shift in perspective is a foundational element in professionalizing the caregiving role, and can help manage the emotional volatility associated with rare disease progression.
Caregiver burnout is a clinical reality in the rare disease space, where care is often required 24 hours a day, 7 days a week. Clinical studies indicate that up to 70% of primary caregivers for children with rare conditions report significant psychological distress. Therefore, self-care must be viewed not only as a luxury but as a medical necessity for the stability of the family unit.
Effective coping strategies for parents of children with rare diseases must include a structured plan for psychological self-preservation. This includes:
By treating mental health as a core component of the treatment plan, parents can mitigate the long-term effects of chronic sorrow and ambiguous loss. For those seeking to understand the broader implications of caregiving on daily life, reviewing daily life guides can provide structured frameworks for balancing medical demands with personal wellbeing.
It is also essential to consult a medical disclaimer when interpreting health-related advice to ensure information is applied safely within a specific clinical context.
The emotional atmosphere of a household is significantly influenced by how information regarding the rare disease is communicated. Maintaining open, age-appropriate transparency with the child is a coping mechanism that builds trust and reduces anxiety for both the parent and the patient.
When parents feel they must "protect" their child from the reality of their condition, it often creates a secondary burden of secrecy. Instead, providing clear explanations about medical procedures and the nature of the condition empowers the child. Research shows that children who are involved in their own care decisions, at a developmentally appropriate level, show higher levels of resilience and better long-term health outcomes.
Utilizing resources from an explainer library can assist parents in translating complex clinical terms into language a child can process. This approach helps normalize the child’s experience, moving the focus away from the "pathology" of the disease and toward a managed way of living.
This transparency should also extend to siblings, who often experience their own unique set of stressors. Statistics show that roughly 30% of healthy siblings in "rare" families report feeling overlooked or anxious about their brother or sister’s health.
A common challenge for parents is the "medicalization" of the home, where the identity of the family becomes entirely defined by the rare disease. A powerful coping strategy is the intentional maintenance of a non-medical family identity. This involves creating "medical-free zones" or times where the focus is strictly on traditional parenting, play, and family development.
While the disease may require 100% of the attention during a crisis, in periods of stability, it is vital to prioritize activities that are unrelated to the diagnosis. This practice helps prevent identity erosion, where the parent forgets they are a person beyond their role as a "caregiver-manager."
Strategies for maintaining identity include:
Maintaining these boundaries helps preserve the parent-child bond, ensuring the relationship is rooted in more than just the administration of care.
The mental energy required to repeatedly explain a rare condition to strangers, extended family, or school officials is a significant source of "decision fatigue" and emotional drain. Creating operational systems and pre-planned response scripts can drastically reduce this cognitive load.
Parents are encouraged to develop a "standard operating procedure" for various social and professional scenarios. For example, having a printed "About Me" sheet for the child that explains the condition, emergency protocols, and common misconceptions can save hours of verbal explanation. Additionally, developing a concise, two-sentence script for casual inquiries allows parents to acknowledge a question without being forced into an emotionally taxing conversation.
Navigating the bureaucratic side of rare disease, such as IEP (Individualized Education Program) meetings or insurance appeals, requires a high level of organization. Understanding the policy and regulation guides can help parents approach these tasks with a professional mindset rather than an emotional one. By systematizing the advocacy work, parents can separate the "task" from the "feeling," which is a core tenet of long-term psychological endurance.
The landscape of rare disease care is evolving, with an increasing focus on the holistic health of the entire family unit. Ongoing research into caregiver resilience is beginning to influence clinical guidelines, suggesting that parental mental health screenings should be integrated into pediatric specialist appointments.
As healthcare systems recognize that the sustainability of pediatric care depends on the health of the caregiver, we can expect more structured support in the form of dedicated mental health grants and specialized clinical trials for family interventions. Collaboration between patient advocacy groups and policy makers continues to highlight the need for systemic changes, such as improved access to home nursing and standardized disability protections.
Ultimately, coping with a rare disease is a marathon that requires a strategic approach to mental and emotional energy. By implementing these five strategies, peer support, mental health prioritization, transparent communication, identity maintenance, and operational systems, parents can build a resilient foundation for their family's future.
For more information on the mission of our organization and our commitment to the rare disease community, please visit our about us page or consult our glossary of rare disease terms for assistance with complex terminology.